Eric L. Johnson, MD Department of Family and Community Medicine, University of North Dakota School of Medicine and Health Sciences; Altru Diabetes Center, Grand Forks, ND ejohnson@medicine.nodak.edu
Dr. Johnson is on the speakers’ bureau of Novo Nordisk and Medtronic Minimed. He received writing assistance for this article from the Med Ed Group, which was funded by Novo Nordisk.
The Journal of Family Practice no longer accepts articles whose authors have received writing assistance from commercially sponsored third parties. This article was accepted prior to implementation of this policy.
Long-term follow-up in the United Kingdom Prospective Diabetes Study (UKPDS) showed ongoing risk reduction for both microvascular and macrovascular complications.22 A separate meta-analysis showed a significant 10% reduction in cardiovascular events with intensive glycemic control when data were combined from the ACCORD trial, ADVANCE trial, VADT, and the UKPDS.23
An improvement in long-term outcomes for patients with T2DM might be expected when initiating a targeted, intensified, multi-factorial interventional regimen to reduce not only HbA1c, but also glucose variability. The STENO-2 trial showed that a targeted multifactorial treatment regimen in patients with T2DM could decrease long-term vascular complications.24
Consider assessing true variability in your patients. Because postprandial glucose levels alone may not equate to overall glycemic variability, you may want to ask select patients to take readings with their glucose meters at various times of the day across several days to get a more accurate picture.5
Implications of glycemic variability
Normal physiologic insulin secretion prevents glucose fluctuations in healthy adults. in patients with diabetes, abnormalities in insulin secretion are part of the pathophysiologic process, resulting in chronic sustained hyperglycemia and acute daily fluctuations in glucose levels. These glycemic disorders are associated with a state of increased oxidative stress and possible subsequent development of vascular complications.
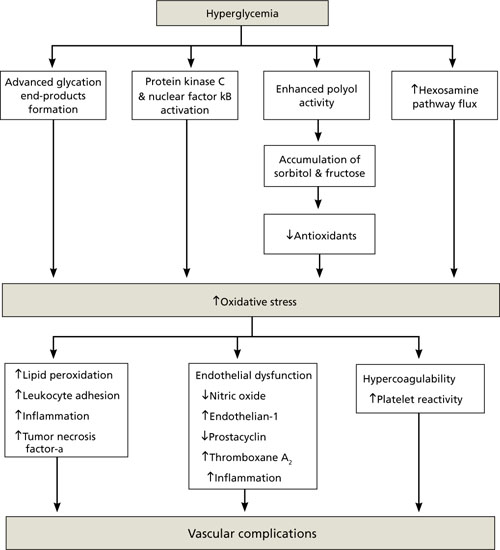
Cellular response to hyperglycemia. oxidative stress, the imbalance between production of reactive oxygen species and the ability to eliminate them, is central to the pathogenesis of cardiovascular complications of diabetes, including accelerated atherosclerotic macrovascular disease (FIGURE 1). Both insulin resistance and hyperglycemia are implicated in the pathogenesis of these complications.65,66 hyperglycemia is hypothesized to induce vascular injury via at least 4 biochemical pathways: enhanced polyol activity leading to sorbitol and fructose accumulation; increased formation of advanced glycation end products; activation of protein kinase c and nuclear factor kB; and increased hexosamine pathway flux.67 endothelium activation is a pro-inflammatory, proliferative, and pro-coagulatory setting, ultimately leading to arterial narrowing and susceptibility to atheroma deposition. hyperglycemia can also induce alterations in the coagulation system, resulting in increased thrombosis.68
Association of glycemic variability with oxidative stress. macrovascular complications, particularly cardiovascular disease, contribute significantly to the increased morbidity and mortality with diabetes.24 oxidative stress has been implicated as a major factor in the development of these complications.66-68 other cell-culture evidence suggests that normal protective mechanisms of oxidative stress are impaired by chronic hyperglycemia. When exposed to intermittent glycemic variability, cells have exhibited more pronounced toxicity.69,70 risso et al71 further established that variability in glycemic control resulted in more endothelial cell damage than did chronic sustained hyperglycemia.
Despite the experimental evidence that suggests glycemic variability is associated with increased risk of vascular complications, there are limited clinical data establishing glycemic variability as an independent predictor of these complications. monnier et al72 provided data in patients with type 2 diabetes mellitus (T2Dm) to support the concept of acute glucose fluctuations as a more important trigger of oxidative stress than chronic hyperglycemia. if these data are confirmed in larger clinical trials, a monitoring paradigm for patients with T2Dm could include increased focus on preventing glucose excursions in addition to reducing HbA1c.
FIGURE 1 How oxidative stress secondary to hyperglycemia leads to vascular complications in diabetes66-68
Following through with targeted, intensified management
Consider the following treatment goals for patients with T2DM: (1) lowering HbA1c levels; (2) lowering fasting blood glucose levels; (3) minimizing glycemic variability, including postprandial glucose excursions. TABLE 1 lists the values that the American Diabetes Association (ADA) and the American Association of Clinical Endocrinologists (AACE) have assigned to these glycemic-control goals.
In addition to managing glycemic levels, reducing risk of cardiovascular disease in T2DM involves aggressive interventions, as needed, to correct blood pressure and lipid levels.24,25
TABLE 1 Aim to reach 3 glycemic goals in treating type 2 diabetes mellitus
ADA
AACE
Fasting blood glucose (mg/dL)
90-130
<110
Postprandial plasma glucose (mg/dL)
<180
<140
HbA1c (%)
<7*
≤6.5
*Recommended “in general”; however, the guideline indicates that for “the individual patient,” HbA1c should be as close to normal (<6%) as possible without causing hypoglycemia.
AACE, American Association of clinical endocrinologists; ADA, American Diabetes Association; HbA1c, glycosylated hemoglobin.
Challenges to achieving glycemic control Despite current recommendations for more aggressive management of patients with T2DM,25 estimates are that as many as 60% of patients with T2DM do not achieve glycemic targets, and, as the disease progresses, many of the available treatment options fail to sustain levels previously reached.1,26,27
A shortcoming of older treatment strategies still in use is the slow transition to more effective therapy, resulting in long periods of inadequate glycemic control.1 Brown et al27 found that patients receiving monotherapy with either a sulfonylurea or metformin had HbA1c levels >8% for a mean of 20 months and 14 months, respectively, before treatment was changed. Current recommendations call for treatment changes within 2 to 3 months of initiation of therapy if the HbA1c goal is not reached.27-29