Eric L. Johnson, MD Department of Family and Community Medicine, University of North Dakota School of Medicine and Health Sciences; Altru Diabetes Center, Grand Forks, ND ejohnson@medicine.nodak.edu
Dr. Johnson is on the speakers’ bureau of Novo Nordisk and Medtronic Minimed. He received writing assistance for this article from the Med Ed Group, which was funded by Novo Nordisk.
The Journal of Family Practice no longer accepts articles whose authors have received writing assistance from commercially sponsored third parties. This article was accepted prior to implementation of this policy.
Long-acting agents Basal, or long-acting, insulins are important for maintaining normoglycemia over 24 hours. Neutral protamine Hagedorn (NPH) insulin reaches its peak effect 4 to 10 hours after injection, and its total effect lasts only 12 to 18 hours. NPH is therefore often dosed twice daily. Absorption of NPH can vary significantly, causing day-to-day blood glucose fluctuations.46,47 Therefore, this agent’s activity does not closely resemble normal physiologic basal insulin secretion.
FAST TRACK
Long-acting insulin analogs stay active up to 24 hours without pronounced peaks, permitting once-daily dosing in many patients.
The newer long-acting insulin analogs—insulin detemir and insulin glargine—were designed to more closely replicate normal physiologic basal insulin secretion. Insulin glargine was first to reach the market, in 2001. It contains glycine instead of asparagine in the alpha-chain and 2 arginine residues at the C-terminus, and the addition of zinc enhances the aggregation and slow release at a neutral pH. Insulin glargine precipitates in the subcutaneous tissue, which slows its absorption and results in a relatively flat insulin plasma profile and extended action.54,55 Insulin detemir is a combination of the original insulin molecule and a saturated fatty acid (myristic acid). Insulin detemir is designed to bind albumin (98% albumin-bound in circulation) through this fatty acid chain in the plasma after injection, resulting in an extended plasma profile.54,56 Insulin glargine and NPH form crystalline depots, but detemir is soluble and the subcutaneous depot remains in a liquid state; this may account for differences in absorption variability.56
FAST TRACK
In head-to-head comparisons, insulin detemir has demonstrated less within-subject variability of blood glucose levels than insulin glargine.
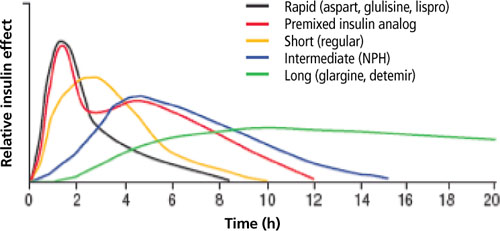
Advantages of the long-acting insulin analogs. Compared with conventional basal insulin such as NPH, the analogs have a prolonged duration of action (up to 24 hours) without pronounced peaks, permitting once-daily dosing in many patients (TABLE 2 and FIGURE 2).46,47,50,55 The pharmacodynamic and pharmacokinetic properties of the long- acting agents make them less likely than NPH to cause nocturnal and overall hypoglycemia, a benefit that has been observed in several clinical trials.57-61
Comparative clinical trials evaluating glycemic variability. Both of the long-acting analogs have shown lower within-subject variability in blood and plasma glucose measurements when compared with NPH.62-64 In head-to-head comparisons of the analogs in glucose clamp studies, insulin detemir has demonstrated less within-subject variability of blood glucose levels than insulin glargine, in patients with T1DM or T2DM.56,64 In clinical practice, different patients may have better results with one of these basal insulins as opposed to the other, and treatment choices will need to be tailored to the individual patient.
TABLE 2 Pharmacokinetic properties giving insulin analogs an advantage over regular insulin46-50
Insulin preparation
Onset of action
Peak action
Duration of action
Short-acting
Regular
30-60 minutes
2-3 hours
8-10 hours
Lispro
5-15 minutes
30-90 minutes
4-6 hours
Aspart
5-15 minutes
30-90 minutes
4-6 hours
Glulisine
20 minutes
90 minutes
5.3 hours
Long-acting
NPH
2-4 hours
4-10 hours
12-18 hours
Glargine
2-4 hours
Relatively flat
Up to 24 hours
Detemir
1-2 hours
Relatively flat
Up to 24 hours
NPH, neutral protamine Hagedorn.
FIGURE 2 Pharmacokinetic profiles of human insulin and insulin analogs
Adapted from: Burton S. J Fam Pract. 2006;55(12 suppl):S10-S17.
CORRESPONDENCE Eric L. Johnson, MD, University of North Dakota School of Medicine and Health Sciences, Department of Family & Community Medicine, 501 North Columbia Road, Grand Forks, ND 58202-9037; ejohnson@medicine.nodak.edu